Phase 4: T3 Thyroid Therapy (Rebooting Your Metabolism)
Where T3 can actually hurt you
T3 raises your heart rate and metabolic demand. At the doses described here it is real medicine with real force behind it. These are the cases where you slow down and build the prep first, and a couple where you get Yannick’s eyes on your numbers before you touch it.
Many people with chronic illness are stuck in a state where their body is “hibernating” to save energy. Even if your blood tests look normal, your body might not be using thyroid hormones correctly. This phase uses a hormone called T3 to “reboot” your body’s thermostat and turn your energy back on.
Is This Therapy Right for You?
Main Requirements (You must have these)
Note: If your resting heart rate is above 90 bpm, resolve that first. An elevated resting HR is a contraindication for starting T3 therapy.
Other Common Symptoms
(Check how many you have – the more you have, the more likely you need this)
- Always tired or waking up exhausted
- Brain fog, trouble concentrating, or memory loss
- Cold hands and feet even when it’s warm
- Gaining weight easily or unable to lose it
- Dry skin or hair that is thinning/falling out
- Feeling low, anxious, or irritable
- Muscle and joint aches
- Frequent headaches or swelling (fluid retention)
Quick Check:
Low Morning Temp + Low Pulse + 3 or more symptoms → You may be a good candidate for T3 therapy.
Track your temp and pulse for one week to be sure.
Getting an Accurate Temperature Reading
Use a Basal Body Thermometer, Not a Standard One
Your waking temperature is one of the most important data points in this entire protocol. A cheap drugstore thermometer that reads to one decimal place is not good enough. You need a thermometer precise enough to detect meaningful shifts, the kind used for tracking fertility windows.
A digital basal body thermometer that reads to two decimal places and holds the result for easy reading
Introduction to T3 Therapy
Overview: This therapy uses T3 (thyroid hormone) to help with fatigue and low body temperature. The goal is to “restart” your metabolism. You can dive deeper into it on this site: wilsonssyndrome.com
The Best Way: Slow-Release T3 (SR-T3)
We strongly recommend using Slow-Release T3 (SR-T3).
- Why? It keeps your hormone levels stable all day and night. It doesn’t cause sudden spikes like regular T3.
- Evening Use: You can take it in the evening to help your metabolism while you sleep.
- Easier to Use: You don’t have to keep taking small doses throughout the day.
Where to Get T3
One trusted source for Slow-Release T3 is chronic-illness.st. They specialize in this medication and can ship to many places. (Previously chronic-illness.ca, the site has recently migrated.)
If you have trouble getting your medication, Yannick can help you find a way to get what you need.
Why Your Blood Tests Might Lie to You
The Real Problem: Tissue-Level Resistance
Most doctors look at your blood to see if you have enough T3. But just because T3 is in your blood doesn’t mean it’s getting inside your cells where it’s needed. This is called tissue-level resistance.
Side-by-side: the same lab result, two completely different cellular realities. This is why “your labs are normal” is not the answer chronic illness patients need.
Think of T3 as a “key” and your cells as “doors.” In many sick people, the locks are jammed. The T3 keys are floating around in the hallway (your blood), but they can’t get into the rooms (your cells) to turn on the power. When a doctor draws your blood, they see plenty of keys and say, “You’re fine!” Even though your body is actually starving for energy.
Brain Insulin Resistance
This problem is especially serious in the brain. When T3 can’t get into your brain cells correctly, it leads to a type of “brain insulin resistance.” This causes major brain fog, memory problems, and severe fatigue. Even if you eat enough food, your brain can’t use that energy properly without the T3 “key” to unlock the process.
Other Signs of Resistance:
- Low Body Temperature: If your cells don’t have enough T3, they can’t create heat. This is why you feel cold even if your blood tests are “normal.”
- High Reverse T3: Sometimes your body makes a “fake key” called Reverse T3 that blocks the real T3 from working.
- Adrenal Stress: When your cells are starving for energy, your body pumps out stress hormones (like cortisol) to try to keep you going. This eventually leads to total burnout.
T3 therapy is used to “electrify” the body, sending a structured “electrical signal flood” of abundance and shock to finally force those jammed locks open and wake your body up. This convinces the cells that T3 can enter again and radically increases insulin sensitivity. Depending on the case, this may require a mix of T4 and high T3, or just T3, but the concept of a short, powerful energy burst remains the same. Do not forget to understand the critical co-factors required for T3 therapy to be safe and effective.
The Role of Genetics: In some cases, your genetics can play a big role in how your body handles T3. Fasting, stress, and low-carb can have different effects on different people. To learn more about this, visit the Genetic Polymorphisms page.
When to Start T3: The Fasting Block Integration
Start T3 on Day 3 of the Water Fast, Not After
In the Scorch Protocol, T3 therapy does not begin at the refeed. It begins on day 3 of the water fast that follows the 5-day dry fast. This timing is intentional.
By starting T3 on day 3 of the water fast, you are on T3 day 3 when you have your first calories. This matters because T3 needs to already be running when refeeding begins It supports your metabolism, keeps your kidneys in a stronger state, and crucially, it means your antiviral protocol (L-lysine + monolaurin) can start immediately on refeeding day 1. You do not need to wait for kidney rehydration before beginning antivirals.
The 30-Day T3 Cycle
This plan is designed to wake up your body’s metabolism. It involves a 10-day “climb” followed by a 20-day “descend.”
| Phase | Time | What to Do |
|---|---|---|
| The Climb | 10 Days | The Hike Up: Increase your total daily dose by about 15 mcg every single day. Example: Day 1 = 15mcg, Day 2 = 30mcg, Day 3 = 45mcg... Note: Split your total dose into two parts: one in the morning and one in the evening. |
| The Peak | 1–3 Days | Stay at your highest dose for a few days to “break” your metabolism’s resistance. If your heart races or you feel anxious, stop increasing. |
| The Taper | 20 Days | The Hike Down: Slowly lower your dose back to zero. This lets your thyroid start making its own hormones again without a crash. |
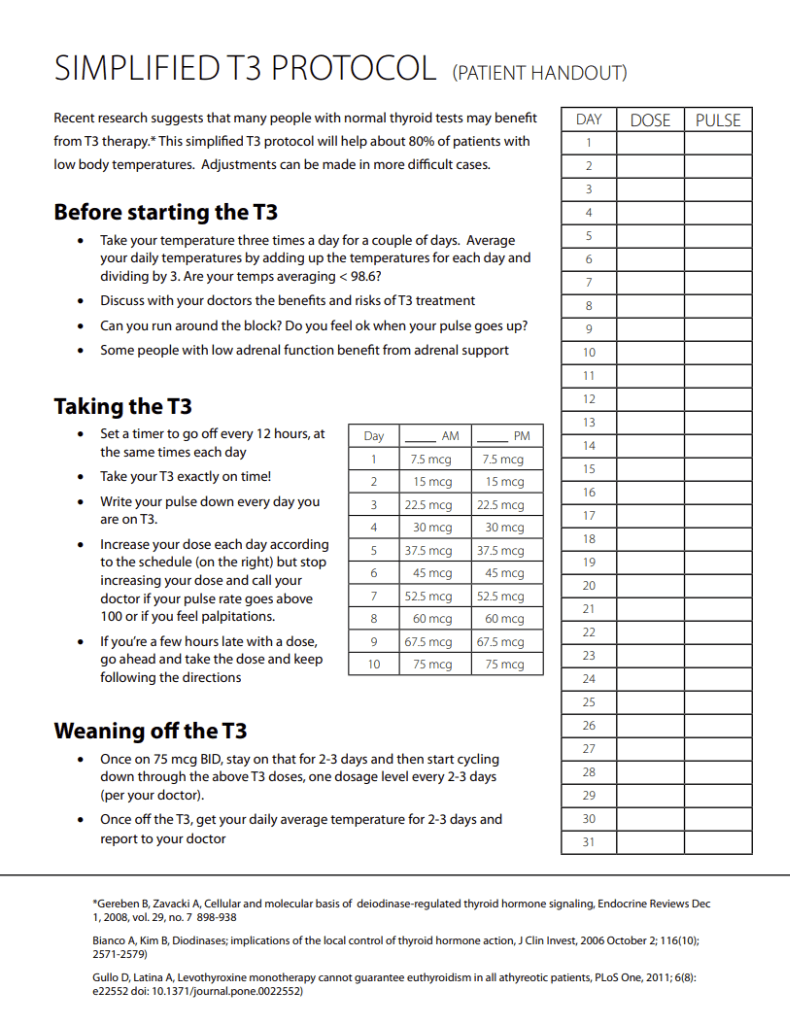
Figure 1: Simplified T3 Protocol Dosing & Tracking Chart
Safety First
Drug Interactions You Need to Know About
Thyroid can thin blood, especially at higher doses. Patients on warfarin sodium (Coumadin®) or other anticoagulants may develop an increase in prothrombin time requiring a lowering of their anticoagulant therapy while taking thyroid medication. Drug-drug interactions may occur with other anticoagulants, oral hypoglycemic agents (increased requirements), insulin (increased requirements), estrogens and oral contraceptives (increased thyroid requirement), tricyclic antidepressants (enhanced effects), cardiac glycosides (potential toxicity and reduced dose) and cholestyramine (decreased T3 and T4 absorption). Several drugs, including cimetidine, ranitidine, glucocorticoids, amiodarone and beta-receptor antagonists, have been reported to increase the hepatic metabolism of T4 into reverse T3 by inhibiting 5’-desiodinase, the hepatic microsomal enzyme catalyzing the conversion of T4 into T3.
Keeping Your Progress
- Supplements: Take B-Complex vitamins, Vitamin C, and electrolytes to help your body.
- Diet: Eat plenty of protein to keep your metabolism strong.
- Bone Health: Take Vitamin K2 to keep your bones healthy during this therapy.
- Success: When you are finished, your waking temperature should stay between 36.5°C and 37.0°C (97.7°F - 98.6°F) without any medicine.
The Co-Factor Stack That Makes T3 Stick
T3 reboots metabolism, but whether it holds depends on three things going right at the same time: you have to eat enough, you have to sleep, and your stress hormones have to come down instead of spiking. The protocol uses a small co-factor stack to protect all three.
None of these replace T3. They are what keep T3 working long enough to reset your baseline.

Figure 2: The ideal body temperature curve of a healthy person, rising through the day and peaking in the late afternoon. If your T3 therapy works, your temperature pattern should begin to match this curve.
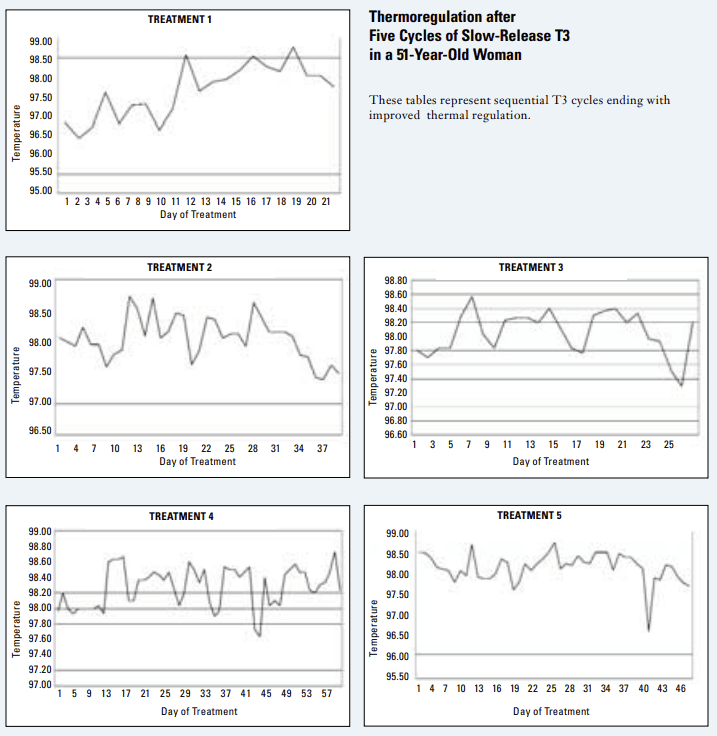
Figure 3: Real-world thermoregulation data across five cycles of slow-release T3 in a 51-year-old woman. Each cycle progressively lifts the waking temperature baseline toward the healthy 36.5 to 37.0°C range shown in Figure 2, the pattern most participants follow when the protocol is working.
Fueling T3 Therapy: Why Calories Matter Here
T3 dramatically increases your metabolic rate. That is the point. But a faster metabolism with insufficient fuel will cannibalize muscle. You must not be in a caloric deficit during this phase.
- hGH: directly shifts the body toward anabolism and preferential fat use, reducing the rate at which muscle is burned for fuel even when calories are temporarily low.
- Retatrutide: a GLP-1/GIP/glucagon triple agonist that improves glucose utilization and raises baseline energy availability. The glucagon component is particularly useful for people stuck in low-energy states.
- Cyproheptadine: the primary first-cycle lever for filling the eating window when appetite is broken or the gut is hypersensitive. It restores the drive to eat, calms the brain-gut nerves that make large meals nauseating, and deepens sleep when repair on T3 happens. For many people this is the single cheapest way to get calories back up early in the refeed. See the stop-before-hGH caveat: cyproheptadine is a first-cycle tool and is stopped before hGH.
Get your own customized refeed plan
Members build a personalized, day-by-day refeed plan: food choices and a calorie ramp sized to their own fast, plus when to layer in T3 and the rest of the protocol. It starts at $1.
Build your refeed plan →Can't actually get slow-release T3?
This is the wall almost everyone hits. No doctor will prescribe slow-release T3, and the peptide and hGH markets are full of fakes. Inside 1-on-1 coaching you get Yannick’s current, personally verified supplier contacts for slow-release T3, peptides, hGH, and cyproheptadine, plus exactly what to order and how to dose it. Most people say that list alone was worth the price.
How the 1-on-1 works →Have a question about your own case?
Ask Yannick directly. Members send their labs, symptoms, and questions and get a personal, reviewed answer, plus help sourcing medication and the full synthesized protocol behind every reply. It starts at $1/mo.
Ask Yannick for $1 →References
- Cahill GF Jr. Starvation in Man. New England Journal of Medicine, 1970. — the fasting-metabolism timeline: the brain's shift to ketones and muscle sparing once ketosis is established, and why T3 must be paired with adequate fuel
- Influence of absolute (dry) fasting on metabolic processes and organ function. — profound insulin suppression and improved insulin sensitivity (HOMA-IR) during fasting
See the full research & citations page for the complete evidence base and how each study is used.